In a recent session at the House of Lords, the topic of out-of-hospital cardiac arrest took centre stage. Baroness Finlay of Llandaff started the session by asking His Majesty’s Government what steps they are taking to improve outcomes in cases of sudden cardiac arrest. Lord Evans of Rainow (Conservative) represented the government and responded to this and the following questions in a 10-minute interaction. Primarily the questions focused on the earlier stages of the Chain of Survival, but thanks to Lord Aberdare (of the APPG Defibrillator group who we have presented to previously), the subject of a care pathway for survivors was raised.
Read the transcript on the government website
The Contributors
Featuring Lord Evans of Rainow (Conservative) responding to questions from the house:
Baroness Finlay of Llandaff (Crossbench)
Lord Hunt of Kings Heath (Labour)
Lord Allan of Hallam (Liberal Democrat)
Lord Moynihan (Conservative)
Baroness Wheeler (Labour)
Lord Sikka (Labour)
Lord Laming (Crossbench)
Lord Murray of Blidworth (Conservative)
Lord Aberdare (Crossbench)
The 80,000 Cardiac Arrests
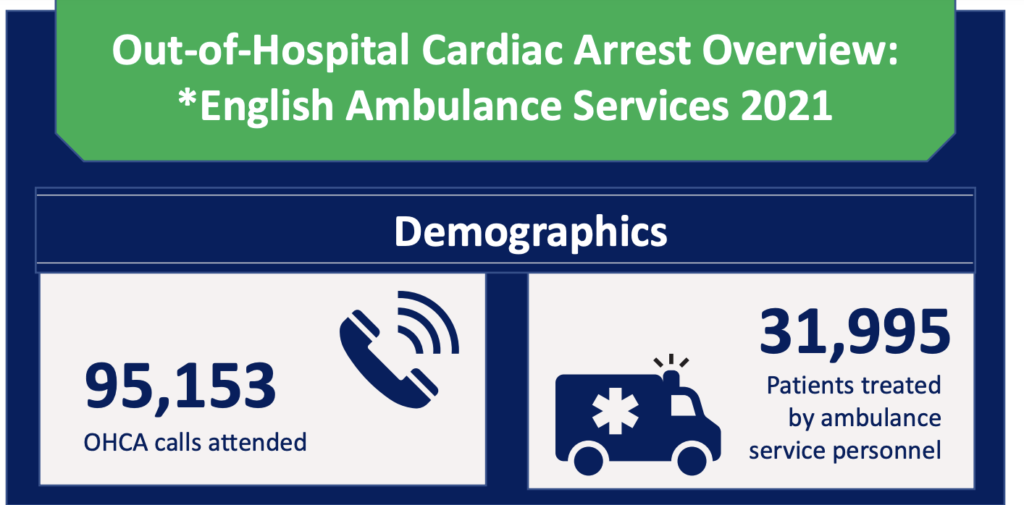
It was stated that approximately 80,000 cardiac arrests occur each year out of hospital, primarily happening in homes. This figure is vastly more than is commonly reported, typically “about/around/approx/above” 30,000.



The 30K is still a large number, but it is well short of the number quoted by Baroness Finlay and just a third of the reported OHCA calls made to Ambulance Trusts in England (2021).
I think the ~30,000 figure is badly misrepresented in many cases and undersells the actual problem. Where that figure is used, it essentially ignores the thousands of others who pass away without treatment. It should be noted that a sizeable proportion of these may be due to DNACPR, or the patient’s death was expected, and I’ve been told that many ambulance trusts do not report the data on these cases. However, we can get an insight into what they might be by looking at the London Ambulance Trust report from 2018-19, where of the 10,152 who had an OHCA, 4,004 (~39%) had resuscitation attempted, 1,762 (~17%) were in the DNACPR or expected group, which leaves 4,386 who did not have resuscitation attempted. In these can be extrapolated to the national figures, then tens of thousands of people are just lost in the “above 30,000” or missed out altogether “30,000”. It’s a crying shame that more emphasis isn’t placed on the higher figures more often.

Comprehensive Care Pathway for Survivors
Lord Aberdare brought up the issue of a post-cardiac arrest care pathway, stressing that survivors often receive inadequate follow-up care compared to other medical emergencies. Establishing a formal care pathway and individualised rehabilitation plans for cardiac arrest survivors is crucial, including support for families and those who perform CPR.
Misconception of Heart Attacks and Cardiac Arrest
In response to Lord Aberdare’s question, Lord Evans of Rainow made the common mistake of confusing heart attacks and cardiac arrest. These are two distinct medical events, and it’s crucial to understand the difference between these terms to address each condition accurately.

A common meme is like the following, which shows the pathological difference,
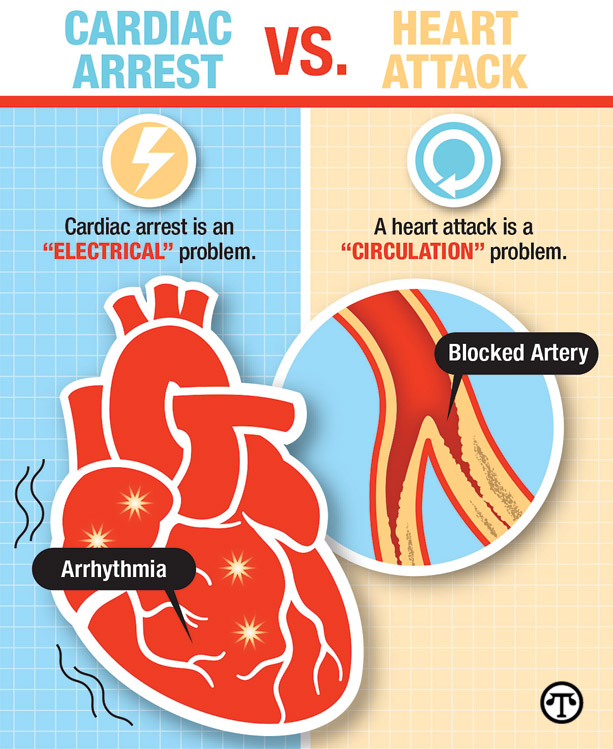
But this misses the crucial point that someone having a heart attack will be conscious and breathing and may be able to help themselves. A person having a cardiac arrest will be unconscious, not breathing, and unable to save themself from a rapidly approaching untimely end. If someone is resuscitated from a cardiac arrest, there is also a good chance they will succumb to some brain and other organ injuries.
Government’s Efforts
The government has recognized the importance of increasing survivorship from cardiac arrest. They have allocated one million pounds for a grant scheme to expand AEDs’ accessibility. Additionally, cardiac first aid training is already a part of the mandatory curriculum for state-funded schools in England. The NHS long-term plan aims to save up to 4,000 lives per year by 2028 through Community First Responders and AEDs.
It’s got to be said that saving 4,000 lives annually by 2028 is quite a big ask – a 60% increase in just five years! Whilst it will be a tremendous achievement if it can be met, it is essential that we have an official care pathway for survivors and co-survivors so that they can return to the best quality of life possible – something that is very hit and miss and the moment.
Disparities in Survival Rates
Data from the UK Out-of-Hospital Cardiac Arrest Outcomes Project revealed disparities in survival rates across regions. For instance, the survival rate after 30 days in London was reported at 11%, while it was only 5.3% in the West Midlands. This stark difference warrants further investigation and intervention in areas with lower survival rates.
If you want to see the statistics for your region, check out the interactive map at the Warwick Clinical Trials Unit.
Defibrillator Registration and Accessibility
The importance of registering defibrillators to ensure emergency services can direct bystanders to their locations during cardiac arrest incidents was highlighted. Also mentioned the need for a unified signing system to identify public access defibrillators better.
Publicly accessible defibrillators should be registered on the Circuit, as is the database the Ambulance Trusts use when you call for help. From the reports I’ve heard, it could be better, but it is what we have and a good start. The more widely used it becomes, the more use CPADs will get; hopefully, more lives will be saved.
Government’s Role in Evidence-based Practice
To ensure consistent and evidence-based treatment across the NHS, the government must prioritise establishing best practices and learning from outstanding hospitals to improve outcomes for cardiac arrest patients.
BCIS Consensus statement on OHCA 1 – Care Pathway
BCIS Consensus statement on OHCA 2 – Post-Discharge Rehabilitation
Role of Food Manufacturers in Cardiovascular Disease
In the context of cardiovascular disease, the role of food manufacturers was questioned, with concerns about excessive salt, sugar, and fat content in food products triggering neurological responses and cravings for unhealthy food. The government’s plans to examine the impact of food manufacturers on cardiovascular disease were sought, but no definitive answer was given.
In Summary
- Formal care pathways and individualized rehabilitation plans should be established for cardiac arrest survivors.
- Rapid intervention is essential for improving survivorship from cardiac arrest.
- In the UK, far more cardiac arrests occur annually out of hospital than is generally publicised, primarily in a home environment.
- The response to Lord Aberdare’s question incorrectly conflated heart attacks and cardiac arrest. With a heart attack, the patient will be conscious and breathing, but in a cardiac arrest, the patient will be unconscious and not breathing.
- The government has allocated funding to expand accessibility to AEDs and already includes cardiac first aid training in the mandatory curriculum for state-funded schools.
- Disparities in survival rates across regions require further investigation and intervention.
- Defibrillator registration and accessibility need improvement.
- The government must prioritise evidence-based practices to ensure consistent treatment across the NHS.
- There are concerns about the role of food manufacturers in creating cardiovascular disease, which may increase the risk of cardiac arrest.

After our first meet-up in February 2015, I realised I was not alone. It was the first time since my cardiac arrest the previous year that I had spoken face-to-face with someone who had experienced what I had. This was also true for my wife, who also happened to be my lifesaver. From that meet-up, the idea of SCA UK was born. Since then, we have achieved a considerable amount, primarily providing information, resources and support to others in a similar situation but also raising the profile of survivorship and the need for better post-discharge care. We are starting to get traction in this, and with the formation of the charity, I genuinely believe we have a bright future ahead and will make a significant difference in the lives of many who join our ranks.